This page contains specialised information intended exclusively for licensed medical professionals. By continuing, you confirm that you are a physician or medical care provider.

Injectable MACT: Matrix-Associated Autologous Chondrocyte Transplantation
Injectable MACT is our injectable treatment for focal defects, based on 20-plus years of Autologous Chondrocyte Implantation (ACI) experience and the use of new biomaterials. In clinical studies and publications, this approach is also described as hydrogel-based ACI or injectable MACI.
.avif)
Indicated for Focal Knee Defects
ICRS grade III–IV lesions, ≥ 2 cm² defect size treated in Phase III trial [1].
Fully Arthroscopic Delivery
Implanted by injection via double-chamber syringe; no arthrotomy, implant trimming, no glue, or sutures required [2].
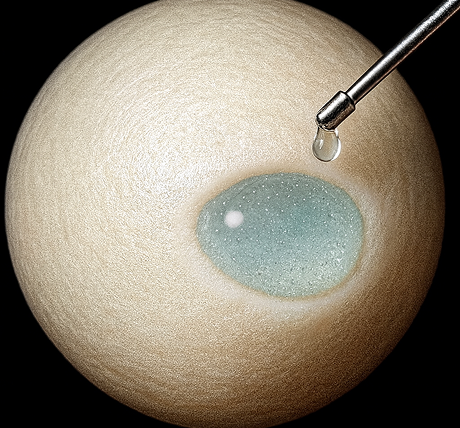
Self-Setting Hydrogel
Injectable MACT solidifies in situ within 1–3 minutes, fixing cells in the defect without coverage [1, 2].
2-Stage Arthroscopic Cartilage Repair
Injectable MACT is an advanced two-stage, arthroscopic ACI treatment for focal, full-thickness cartilage lesions of the knee (ICRS grade III–IV) with a minimum size of 2 cm². In clinical trials, lesions up to 12 cm² were treated successfully [2]. The Injectable MACT approach uses patient-derived chondrocytes embedded within a hydrogel that solidifies in situ and adheres to the lesion without sutures or glue, supporting cartilage regeneration.
Distinct Properties
01
≥ 2 cm² Focal Defects
Treat a wide range of defect sizes with one procedure [1].
02
Available as Outpatient Procedure
With a stable patient and no complications, same-day discharge is possible [3].
03
Shorter Operative Time
Solidifies within 1–3 minutes, eliminating the need for sutures or glue.
04
Hydrogel Matrix
Preserves chondrocyte viability and spherical morphology, offering ideal conditions for cartilage regeneration.
View the Procedure Step by Step
This video demonstrates the intraoperative application of Injectable MACT, including defect preparation and in-situ gel formation.

Indications
Injectable MACT is indicated for patients with:
- Focal, full-thickness chondral or osteochondral lesions of the knee measuring ≥2 cm² (ICRS grade III–IV) [1]
- Closed growth plates
- Stable joint structures
- Minimal malalignment
Contraindications include advanced osteoarthritis (Kellgren–Lawrence grade >2), inflammatory arthritis, or uncorrected malalignment >3°.
Undesirable Effects
The following adverse effects are related to Injectable MACT [1]. Please visit the Physicians Resources page for further information.
Graft-Related Effects
Graft failure, including graft hypertrophy.
Treatment Failure
Treatment failure may occur; approximately 1% at 5 years.
Muscle Atrophy
Muscle weakness or temporary loss of strength around the treated joint.
Pain, Stiffness, Nerve Irritation
Joint pain, stiffness, nerve irritation, muscle atrophy, or blood clots may occur.
Joint Symptoms
Joint swelling, effusion, synovitis, or crepitation may occur.
Long-term outcomes beyond 5 years are not available yet.
Interested in Discussing Injectable MACT?
Explore whether Injectable MACT aligns with your practice.
Understanding the Process

Cartilage Biopsy
Performed arthroscopically through standard portals
3 cartilage-bone cylinders are harvested from a non-load-bearing site (e.g., intercondylar notch)
Tissue is sent to TETEC for culture and hydrogel preparation
Arthroscopic Implantation
Performed arthroscopically using two portals
Defect is debrided to healthy cartilage margins and cleaned
Chondrocyte suspension + crosslinker are mixed and injected directly into the defect
The hydrogel forms in situ within 1–3 minutes—no sutures, glue, or pins required
Joint is cycled to confirm graft stability before closure

Recovery and Rehabilitation
Standard rehabilitation is defect-location based and DGOU-oriented. It requires 48 hours without knee mobilisation before controlled joint movement can be initiated [1].
For load-bearing femoral condyle defects, partial weight-bearing is limited to a max of 20 kg during weeks 1–6. Two forearm crutches are used until full weight-bearing is achieved [1].
For patellar or retropatellar defects, full weight bearing is generally permitted, with a ROM brace and flexion limits determined by defect size and location [1].
Clinical Outcomes
Clinical studies indicate consistent benefits from early recovery through long-term follow-up. The following summary highlights key findings from functional scores and imaging studies.

How We Expand Cells
Trace every step of Injectable MACT manufacturing—from biopsy to graft preparation—and see how controlled environments and human oversight ensure consistent implant quality.
Why Choose Injectable MACT?
Contact TETEC
1. TETEC AG. Fachinformation NOVOCART Inject. Reutlingen (DE): TETEC AG; 2022. Stand der Information: 12/2022. PEI.A.11763.01.1.
2. Niemeyer P, Hanus M, Belickas J, László T, Gudas R, Fiodorovas M, et al. Treatment of large cartilage defects in the knee by hydrogel-based autologous chondrocyte implantation: two-year results of a prospective, multicenter, single-arm phase III trial. Cartilage. 2022;13(1):19476035221085146. doi:10.1177/19476035221085146.
3. Gemeinsamer Bundesausschuss. Beschluss über eine Änderung der Richtlinie Methoden vertragsärztliche Versorgung: Matrixassoziierte autologe Chondrozytenimplantation am Kniegelenk. Berlin (DE): G-BA; 17. Februar 2022.
4. Niemeyer P, Hanus M, Belickas J, László T, Gudas R, Fiodorovas M, et al. Treatment of large cartilage defects in the knee by hydrogel-based autologous chondrocyte implantation: a 5-year follow-up of a prospective, multicenter, single-arm phase III trial. Cartilage. 2025. Epub ahead of print. doi:10.1177/19476035251334737.
5. Richter J, Schuster P. Arthroskopische ACT: die nächste Generation der Knorpelzelltransplantation. Sportärztezeitung. 2016:48–50.